
How to Diagnose Acquired Adult Flat Foot
This Clinical Practice Guideline (CPG) is based on the review of clinical literature and consensus of current clinical practice.

What is Acquired Adult Flat Foot?
Flat feet are not usually painful, especially in children. This condition describes a painful, progressive flatfoot deformity in adults. It is due to a gradual stretching of the main ligaments that support the arch of the foot, as well a slowly worsening stretching (or attenuation) of the posterior tibial tendon.
Who gets this condition?
Adults! Women are four times as likely to get it as men. The most common age group is between 45-65. Usually, people who get this condition have had non-painful flat feet for most of their adult life. Factors such as diabetes, hypertension (high blood pressure) and obesity tend to increase the risk of getting this condition.
What are the signs and symptoms?
Most patients notice gradual worsening pain in one foot, and a gradual flattening of the arch in the affected foot. Pain is usually on the inside, due to pain in the stretching tendons and ligaments, but it is often accompanied by pain on the outside of the ankle, due to compression of the joints on this side. If the posterior tibial tendon ruptures, deformity can progress quickly, until the foot literally dislocates outward from under the ankle joint. This is not good. Really not good.
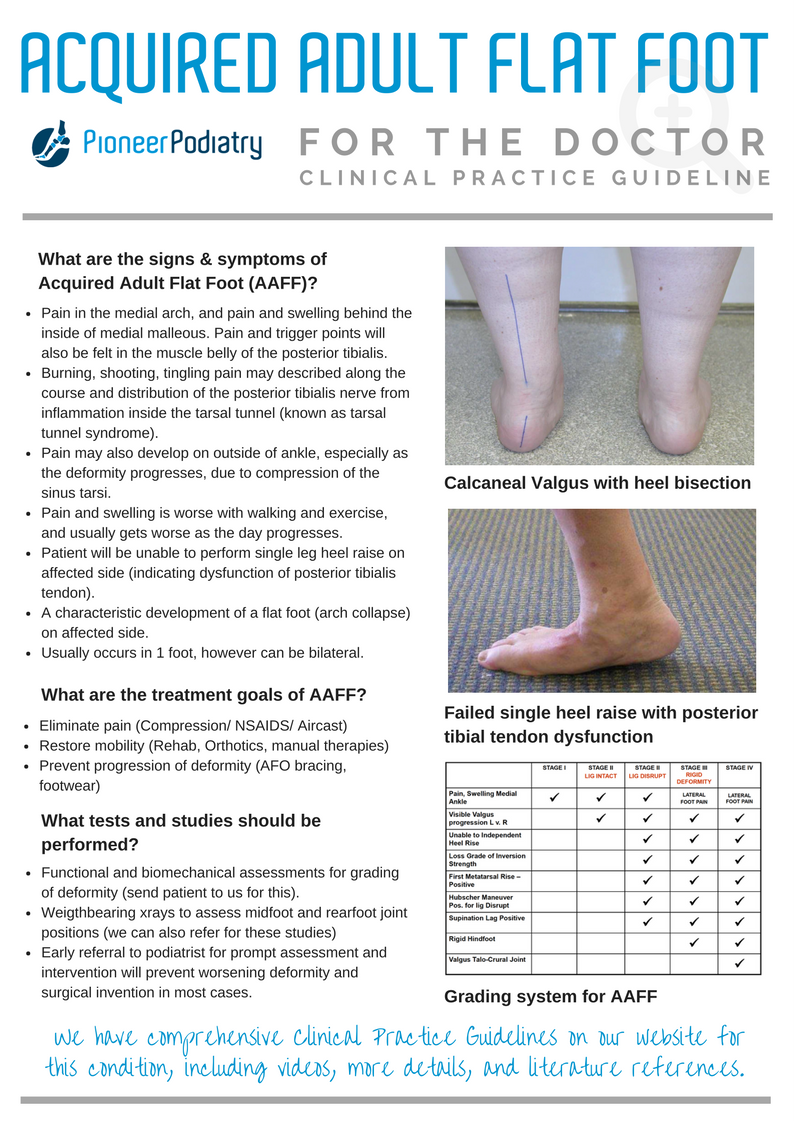
- Pain in the medial arch, and pain and swelling behind the inside of medial malleous. Pain and trigger points will also be felt in the muscle belly of the posterior tibialis.
- Burning, shooting, tingling pain may described along the course and distribution of the posterior tibialis nerve from inflammation inside the tarsal tunnel (known as tarsal tunnel syndrome).
- Pain may also develop on outside of ankle, especially as the deformity progresses, due to compression of the sinus tarsi.
- Pain and swelling is worse with walking and exercise, and usually gets worse as the day progresses.
- Patient will be unable to perform single leg heel raise on affected side (indicating dysfunction of posterior tibialis tendon).
- A characteristic development of a flat foot (arch collapse) on affected side.
- Usually occurs in 1 foot, however can be bilateral.
What tests and studies should be performed?
- Functional and biomechanical assessments for grading of deformity (send patient to us for this).
- Weightbearing xrays to assess midfoot and rearfoot joint positions (we can also refer for these studies)
- Early referral to podiatrist for prompt assessment and intervention will prevent worsening deformity and surgical invention in most cases.
Single leg heel raise- determines the integrity of the plantar midfoot ligaments and posterior tibial tendon

Successful single leg heel raise test.

Failed single leg heel raise test. Note: Midfoot collapse and MT joint flexion.
"Too many toes" sign. Indicates abduction of the forefoot on the rearfoot.

The "Too many toes" sign.
Video explaining how to test for tibialis posterior tendon pathology

Test for posterior tibial muscle strength and tendon integrity

Hubscher's Maneuver- to assess function of the windlass mechanism

The plantar midfoot ligaments- The primary ligament dysfunction in AAFF occurs in the spring ligament.

Differences in talar osseous joint angles in the posterior facet between patients with AAFF and patients without AAFF


How to grade Acquired Adult Flat Foot

What are the treatment goals of AAFF?
- Eliminate pain (Compression/ NSAIDS/ Aircast)
- Restore mobility (Rehab, Orthotics, manual therapies)
- Prevent progression of deformity (AFO bracing, footwear)
Treatment protocols
These treatment protocols are complex and require management by a podiatrist to provide treatment and review progress and modify as appropriate.
Stage I
- Temporary Immobilisation-Support
- Unna Boot
- High-Dye Taping
- Lace-Up brace with Figure 8 straps, favoring inversion
- Physical Therapy with modalities to reduce inflammation
- Footwear Modification
- Follow up custom functional foot orthoses
Stage II
- Temporary Support
- Walking Boot for 1-6 weeks
- Long Term Support
- Footwear Modification
- Functional rehabilitation program 12 weeks
- Custom Hinged Ankle-Foot Orthosis
- Range of Motion, Eccentric strengthening, Balance Training
Stage III
- Temporary Immobilization
- Rarely necessary
- Long Term Immobilization
- If no severe DJD in Ankle and Hindfoot:
- Restricted Hinge AFO with Arch Suspender
- If severe DJD in Ankle and Hindfoot:
- Gauntlet with flexible AFO Shell
- If severe DJD in Ankle and Hindfoot:
Stage IV
- Gauntlet with Solid AFO Shell

Starting position for posterior tibial muscle strengthening exercise. 8-10 reps, 3 sets. Increase resistance to fatiuge.

Instruct patient to plantarflex and adduct foot against theraband, slowly with control, and slowly back to starting position.
AFO bracing for AAFF
The primary treatment for stages II, III, and IV AAFF is custom AFO bracing to reduce pain, restore mobility and prevent progression of deformity.
Our Podiatrist have specialised training in the assessment, design, fitting and management of using custom AFOs for the treatment of AAFF.


Gait analylis showing before and after fitting of custom AFO for left sided AAFF. Note: reduction of forefoot adduction, and calcaneal valgus. The gait parameters in this patient were drastically improved and much more symmetrical.

Before and after gait stills, with the Richie Brace. Note: Obvious improvements in frontal plane foot position, and this patient was able to walk and work pain free almost immediately with this brace.
Studies on the conservative treatment of AAFF
Chao W; Wapner KL; Lee TH; Adams J; Hecht PJ: Non-operative management of posterior tibial tendon dysfunction. Foot Ankle Int. 17(12): 736 – 41, 1996. Alvarez RG; Marini A; Schmitt C; Saltzman CL: Stage I and II posterior tibial tendon dysfunction treated by a structured non-operative management protocol: an orthosis and exercise program. Foot Ankle Int. 27(1): 2 – 8, 2006.
Augustin JF; Lin SS; Berberian WS; Johnson JE: Non-operative treatment of adult acquired flat foot with the Arizona brace. Foot Ankle Clin. 8(3):491 – 502, 2003.
Johnny L. Lin, MD; John Balbas, MD; E. Greer Richardson, MD.Results of Non-Surgical Treatment of Stage II Posterior Tibial Tendon Dysfunction: A 7- to 10-Year Followup Foot & Ankle International/Vol. 29, No.8/August 2008
Krause F, Bosshard A, Lehmann O, Weber M. Shell brace for stage II posterior tibial tendon insufficiency. Foot Ankle Int 29 (11): 1095-1100, 2008.
Kulig K, Reischl SF, Pomrantz AB, Burnfield JM, Mais-Requejo S, Thordarson DB, Smith RW Nonsurgical management of posterior tibial tendon dysfunction with orthoses and resistive exercise: a randomized controlled trial. PHYS THER.2009; 89: 26-37
Nielsen MD, Dodson EE, Shadrick DL, Catanzariti AR, Mendocino RW, Malay DS. Nonoperative Care for the Treatment of Adult-acquired Flatfoot Deformity. Jour Foot Ankle Surg 50 (2011)311-314.
Downloads

Patient Info Sheet for Acquired Adult Flat Foot
Clinical Practice Guideline for Acquired Adult Flat Foot
